Rosie’s Coil
Lorenzo’s Oil in the AI Era

Claudius Papirus, the animated YouTube channel narrated by Claude Opus—the same channel that brought Knuth’s exuberant report about Claude and Schwartz’s “Vibe Physics” to my attention—led me to Rosie’s story. My initial Google search surfaced an older UNSW piece at the top rather than the much improved March 2026 update by the same writer. I tracked down the primary text sources because YouTube transcripts are riddled with timestamps and typos, and what I found was a story considerably richer than the feel-good headline suggested: an AI-assisted citizen science project that compressed what the Odones did with index cards and journal stacks in the 1980s into months, with a beloved pet’s life in the balance.
Gemini provided the technical scaffolding the media coverage largely omitted. It surfaced the cost breakdown, which is sure to dash the hopes of readers inspired by Rosie’s story: sequencing runs $1,000–$3,000, bioinformatics analysis $5,000–$20,000 (which Paul bypassed by acting as his own analyst for 50–60 hours), and bespoke mRNA manufacturing $50,000–$250,000 in a commercial setting. Rosie’s case worked because UNSW’s RNA Institute treated it as a proof-of-concept for human personalized medicine, essentially donating the manufacturing layer. Gem also flagged that KAIST and the Catholic University of Korea are working on related neoantigen prediction projects—context that GPT built on to analyze my medical tourism idea later in the discussion.
Claude landed the sharpest critique of the regulatory framework. The ethics approval took three months of daily work—“arguably more work than the vaccine design itself”—while Rosie’s cancer progressed. The rules assume scarcity and gatekeeping that no longer match technical reality—genomic sequencing now costs $3,000 instead of billions, mRNA vaccines can be designed in weeks, and informed individuals can execute bioinformatics analysis with AI assistance. When I raised medical tourism as a potential workaround for patients facing bureaucratic rather than cost barriers, Claude anticipated the obvious objections (regulation arbitrage, unsafe therapies) and defused them: outcome tracking and quality standards are solvable, and the US government in particular has no credible standing to block citizens from seeking experimental treatments abroad when it neither provides healthcare nor prevents insurers from denying coverage as a matter of routine.
GPT’s most valuable contribution was reframing all the work that Conyngham actually put in. The March UNSW piece finally made the workflow visible—150 billion letters of genomic data, AI-assisted neoantigen identification, iterative hypothesis and validation loops, three months of ethics navigation, finding a specialist willing to administer when local vets couldn’t. That’s not “guy plus ChatGPT equals miracle”; that’s motivated operator plus AI plus institutions producing an outcome. The Project Rosie workspace Conyngham set up on ChatGPT, visible in the accompanying video, is the tell: this wasn’t chat to answer but workspace to pipeline. GPT then developed the medical tourism angle into something more concrete when I mentioned KAIST: better neoantigen target selection reducing failed responses, combined with Korea’s existing strengths in high-skill clinical infrastructure and medical tourism experience, points to a distributed precision medicine pipeline where AI improves target selection, hospitals coordinate execution, and international patients access the result. The limiting factor isn’t talent—it’s permissions and manufacturing partnerships. Whoever solves that layer wins.
The Lorenzo’s Oil parallel holds at every level. Augusto Odone was a World Bank economist; Paul Conyngham is an electrical engineer and AI consultant. Both had cognitive surplus and financial floor sufficient to spend months in technical domains they hadn’t trained in. Both found an institutional insider willing to manufacture what they’d designed—a British chemical company for erucic acid, UNSW’s RNA Institute for mRNA. Facing establishments that told them the diagnosis was a finality, both treated it as a data problem instead. The difference is that AlphaFold compressed years of protein crystallography into hours, and ChatGPT replaced the National Library of Medicine’s physical stacks with a structured knowledge workspace. The underlying dynamic—informed and tenacious amateur bypassing gatekeepers because institutional timelines don’t match survival windows—is identical. What’s changed is the speed, and the implication of that speed is what the media coverage keeps failing to name: this isn’t democratization, it’s a compression of what’s possible for people with the means, resolve, and technical literacy to attempt it. The gap between Conyngham and most pet owners, or most terminal patients, remains vast. Rosie’s story is a glimpse of what medicine could look like for everyone, although it isn’t that yet.
[This post was drafted with assistance from Claude Sonnet 4.6, following conversations with ChatGPT-5.3, Gemini 3 Thinking, and Claude Sonnet 4.5.]
Prompt: My earlier Google search did not serve me well. It showed that earlier UNSW piece at the top instead of this March one, which is much better (same writer, surprisingly, but massive improvement).
Prompt: Yes, in the video, they showed his screen where he had a project set up on your platform specifically for Rosie. That’s the real story. And it’s really ironic that he spent more time struggling with bureaucratic details. Oy. Somehow you can put sick pets to sleep but you can’t try a novel treatment.
Prompt: My earlier Google search did not serve me well. It showed that earlier UNSW piece at the top instead of this March one, which is much better (same writer, surprisingly, but massive improvement). A bit more insight into Paul’s process. There was even an accompanying video clip, where they showed his GPT page where he’d set up a “Project Rosie.” Much smarter approach, although people who are inspired by this story might get a major sticker shock now, because the genome sequencing fee is not mentioned at all.
Seems the story broke out in the US a few weeks ago, with both NBC and CBS interviewing Conyngham. Rosie looked healthy to me (but I’m not a dog owner) and not too frail. Really funny how outlets describe Conyngham differently: Claudius said he was a data scientist, Fortune and NBC a tech entrepreneur, and CBS an AI expert. I think UNSW’s description is probably the most accurate, since they interviewed him closely twice. So no biomedical expertise, but certainly knows how to analyze data and has the doggedness and tech savvy to wade through massive strings.
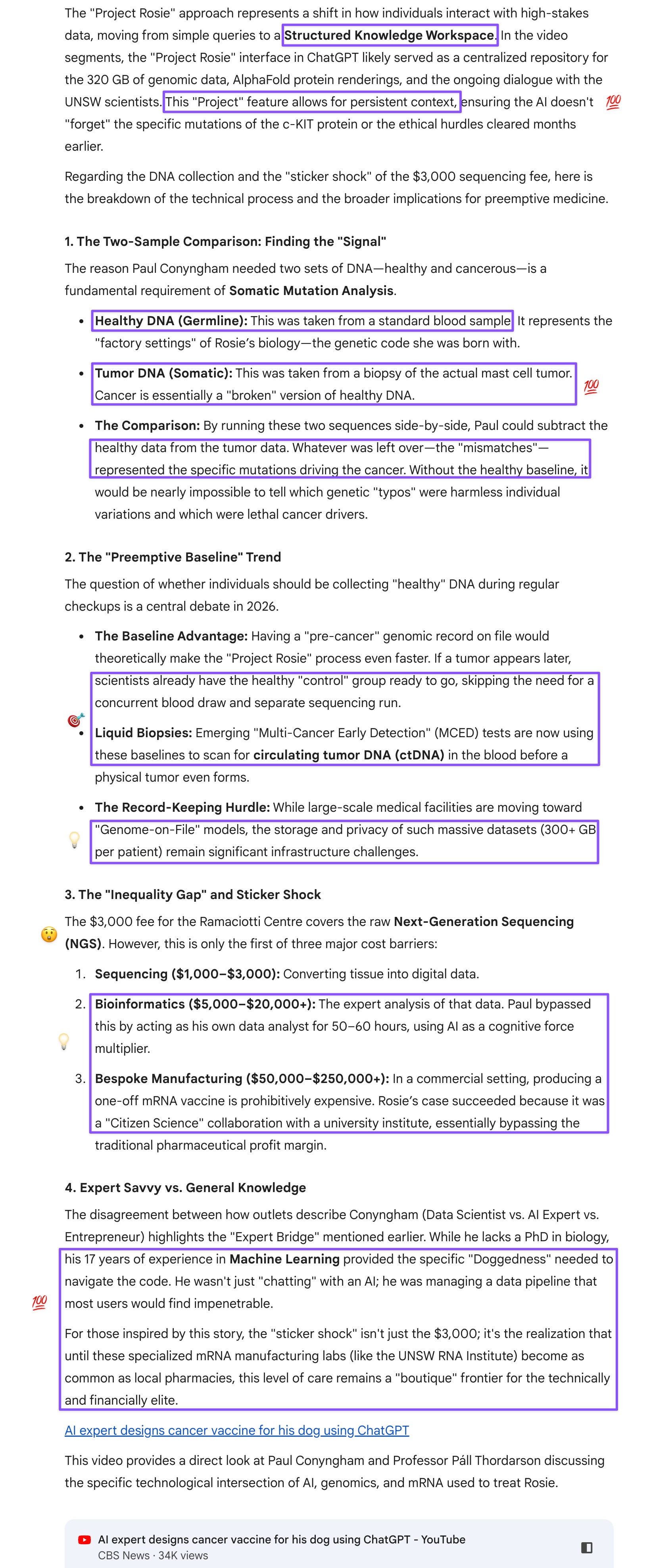
I was curious how Conyngham had Rosie’s healthy DNA as well as the current one. Is this something that people should now be doing for themselves and their pets, or that the medical facilities should be collecting at regular checkups and preserving on record so they could be used in a case like Rosie’s?
Prompt: This discussion was so interesting I almost forgot a pre-AI analogue: Lorenzo’s Oil!
Prompt: It’s really ironic that he spent more time struggling with bureaucratic details. Oy. Somehow you can put sick pets to sleep but you can’t try a novel treatment. Really shows regulators are not keeping up and being almost derelict in their duties.
Prompt: Gem gave me the fee schedule. Seems a bit irresponsible for the media not to mention this. And most insurances aren’t going to cover experimental trials anyway, so individuals have to pay out of pocket, unless their case is scientifically interesting.
The “Inequality Gap” and Sticker Shock
The $3,000 fee for the Ramaciotti Centre covers the raw Next-Generation Sequencing (NGS). However, this is only the first of three major cost barriers:
1. Sequencing ($1,000–$3,000): Converting tissue into digital data.
2. Bioinformatics ($5,000–$20,000+): The expert analysis of that data. Paul bypassed this by acting as his own data analyst for 50–60 hours, using AI as a cognitive force multiplier.
3. Bespoke Manufacturing ($50,000–$250,000+): In a commercial setting, producing a one-off mRNA vaccine is prohibitively expensive. Rosie’s case succeeded because it was a “Citizen Science” collaboration with a university institute, essentially bypassing the traditional pharmaceutical profit margin.
I guess people could raise money through GoFundMe, although if regulations don’t keep up with the technology, people are going to get stuck like Parkinson’s patients waiting for stem cell research to happen.
Prompt: Conyngham is like the AI-assisted version of Lorenzo’s parents.
Had another shot-in-the-dark thought. Resource-poor but technically advanced countries could soon offer a bespoke end-to-end medical tourism service for patients or pet owners who only face a bureaucratic barrier? And as supplies expand, then the costs could become more affordable as well?
Prompt: The EU throwing out roadblocks, I’d understand. The US, no. Even the don’t-tread-on-me crowd won’t take kindly to a government (that doesn’t provide healthcare unlike EU countries or mine or prevent insurance companies from denying coverage as a matter of routine) telling them what to do on matters of life and death :D
Prompt: Here’s a thought. My country is poor in natural resources but has terrific human ones. Medical tourism is a sector that seems to be doing well. Isn’t this something that medical establishments like my country’s could work with?
Prompt: My people are certainly enterprising :D Check out “KAIST”!